- Home
- pms nervousness
- PDF] Premenstrual syndrome, a common but underrated entity: review of the clinical literature
PDF] Premenstrual syndrome, a common but underrated entity: review of the clinical literature
5 (467) · $ 18.00 · In stock
![PDF] Premenstrual syndrome, a common but underrated entity: review of the clinical literature](https://d3i71xaburhd42.cloudfront.net/ca4746c4e9f26db0e1dbf7c0084a6ef3f4da138c/14-Table1-1.png)
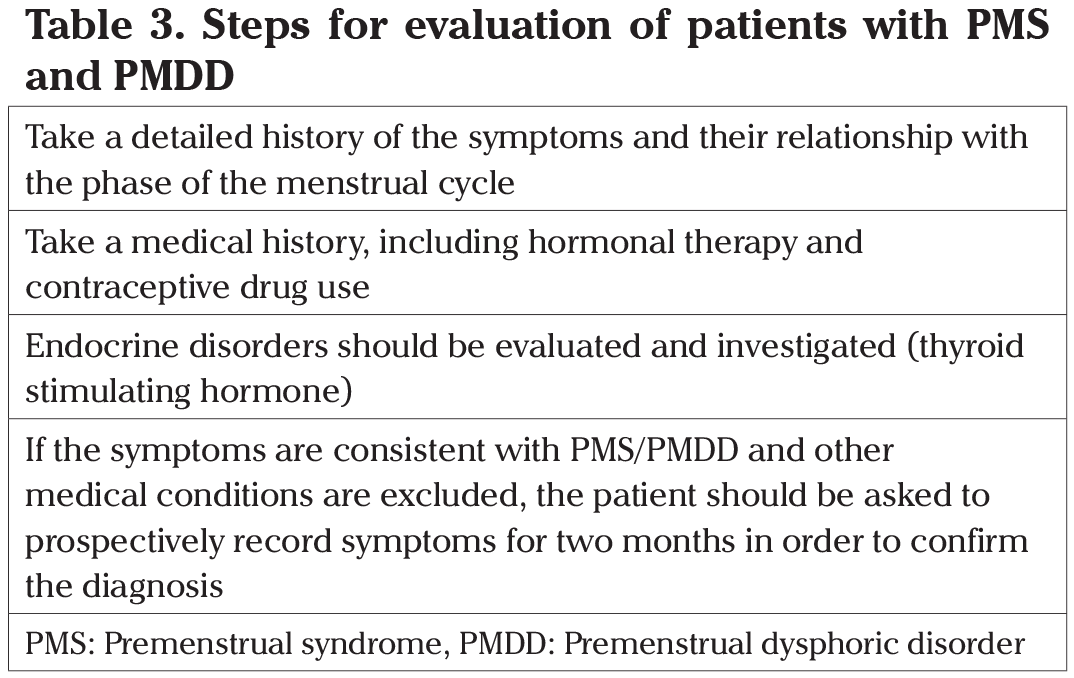
Drugs that suppress ovarian sex steroid production, such as combined oral contraceptives or selective serotonin re-uptake inhibitors enhancing central serotonin delivery are used for treatment and life-style changes and regular exercise also have a positive effect in milder cases. Premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD) are characterized by somatic and psychologic symptoms that arise at the luteal phase of the menstrual cycle and subside with menstruation. For definitive diagnosis prospectively self-reported symptoms should demonstrate a cyclic pattern and other psychological pathologies and thyroid dysfunction, that may present with similar symptoms, should be excluded. Both entities affect millions of women at reproductive age as the prevalence of PMS is given as 10-98% while PMDD affects 2-8%. Sex steroids and neurotransmitters have a central role in the etiology. The role of vitamins and minerals in the etiology and treatment of PMS and PMDD is open to discussion. Drugs that suppress ovarian sex steroid production, such as combined oral contraceptives or selective serotonin re-uptake inhibitors enhancing central serotonin delivery are used for treatment. Life-style changes and regular exercise also have a positive effect in milder cases. Tricyclic antidepressants and gonadotropin-releasing hormone analogues can be used in selected cases.

Premenstrual dysphoric disorder: Video & Anatomy

Frontiers Academic and Social Impact of Menstrual Disturbances
Journal of the Turkish-German Gynecological Association
Nutritional practices to manage menstrual cycle related symptoms
PDF) Premenstrual Dysphoric Disorder: A Review for the treating
The effect of a social network-based cognitive behavioral therapy
The premenstrual defence - Futurum
PDF) Premenstrual syndrome, a common but underrated entity: Review
PDF) Impact of nutritional diet therapy on premenstrual syndrome